- Mon - Sat: 9:00
- Call Us: +90 (538) 894 00 91
- [email protected]
Femoroacetabular Impingement
Due to morphological abnormalities in the hip joint, it is the pathological contact and impingement that develops between the femoral head-neck junction and the acetabulum. Three types of femoroacetabular impingement have been described: CAM type, Pincer type, and Combined type.
Secondary damage within the joint (labral tears and cartilage damage) caused by impingement can lead to a clinical condition causing hip pain in patients. This clinical condition is referred to as femoroacetabular impingement syndrome. The pathophysiological process developing within the joint due to impingement is considered a risk factor for hip osteoarthritis (joint degeneration) in the long term.
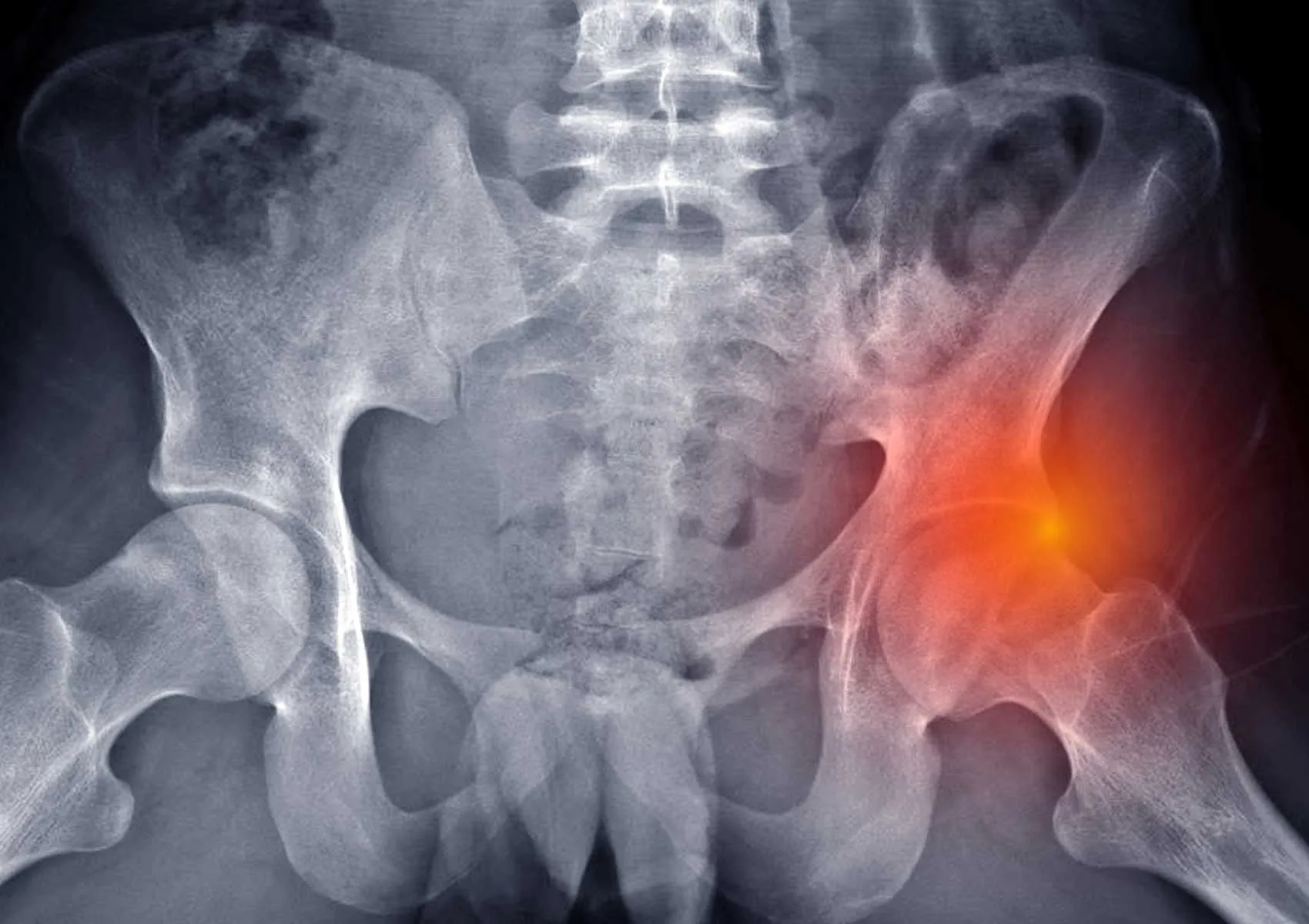
CAM type impingement is caused by the femur. Typically, there is a bony prominence (CAM lesion) on the anterolateral (front-side) aspect of the femoral neck. This causes a shearing force within the joint as the femoral head enters the acetabulum. This impingement leads to extensive labral tears and cartilage damage. It is more commonly seen in young male patients. (Figure 1)
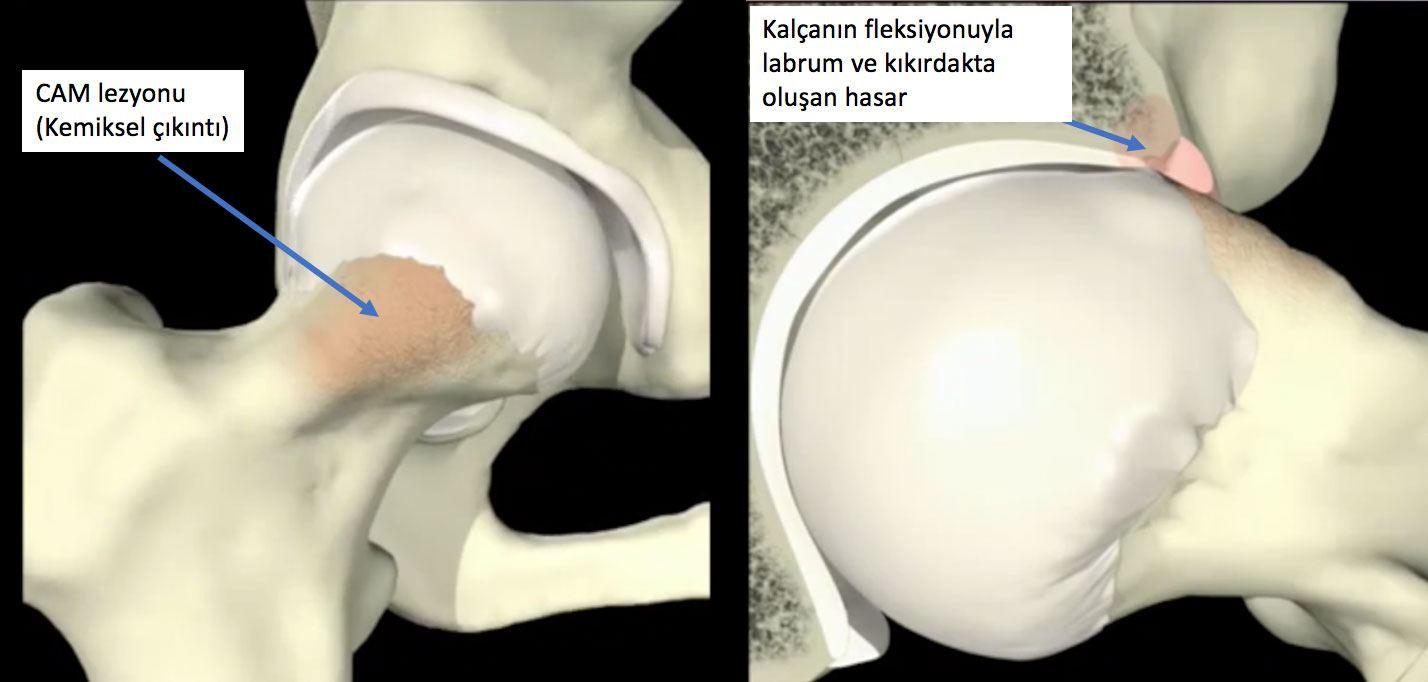
Figure 1: The bony abnormality causing CAM type impingement and the damage occurring during joint movement are shown.
It develops due to excessive coverage of the acetabulum. It is more commonly seen in middle-aged female patients. Secondary damage in the joint develops more slowly compared to CAM type. (Figure 2)
Figure 2: The bony abnormality causing Pincer type impingement and the damage occurring during joint movement are shown.
This is the type where both impingement types are seen together. It is the most commonly encountered type of impingement.
Patients experience restricted hip movement and pain due to bony deformities and clinical symptoms. Typically, patients have groin pain radiating to the lateral hip, triggered by activity. The pain can be dull or sharp in character. Complaints often increase with activities such as sitting and standing.
Athletes (e.g., football players, bodybuilders), individuals carrying heavy loads, and those with a history of hip joint disease during childhood are more frequently affected.
The diagnosis can be made through X-ray examinations following an evaluation by an experienced orthopedist. Magnetic resonance imaging (MRI) is highly useful for visualizing secondary damage in the joint.
In individuals where non-surgical treatment fails, surgical treatment should be applied. Femoroacetabular impingement is the most common clinical condition for which hip arthroscopy is used today. Through treatment applied via 3-4 portals (entry points), in addition to repairing damaged structures within the joint, it is possible to fully arthroscopically address the Pincer lesion (shaving of the acetabulum, acetabuloplasty) and the CAM lesion (shaving of the femoral head-neck junction, femoroplasty) causing impingement. (Figures 3-4) In experienced hands, clinical success rates after arthroscopic treatment of patients are in the 90% range for 2-5 years.

Figure 3: Hip arthroscopy
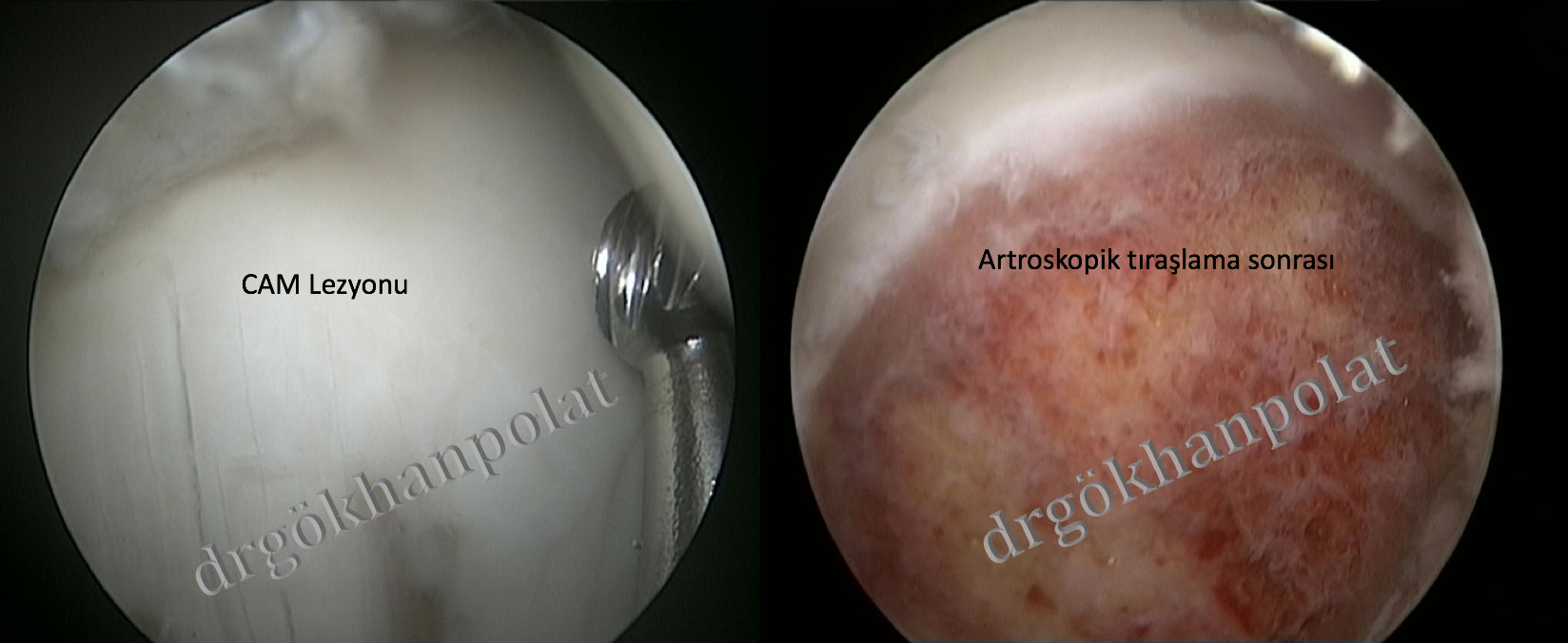
Figure 4: Treatment of the CAM lesion with hip arthroscopy
Prof. Dr. Gökhan Polat Istanbul University Faculty of Medicine Department of Orthopedics and Traumatology
© Prof. Dr. Gökhan Polat | Orthopedics and Traumatology Specialist - All content on this website belongs to Prof. Dr. Gökhan Polat. Unauthorized copying is prohibited.