Femoroacetabular Impingement: Symptoms and Importance of Early Diagnosis
Femoroacetabular impingement (FAI) occurs when structural incompatibility between the bones forming the hip joint causes them to rub or pinch each other during movement. This progressive condition, especially seen in young and active individuals, can lead to permanent joint damage if left untreated. The disorder is a common cause of hip pain and was the subject of Prof. Dr. Gökhan Polat’s specialty thesis. Early diagnosis is crucial for the success of joint-preserving surgical approaches. Having a general awareness of hip joint disorders and femoroacetabular impingement helps ensure proper management of the condition.
What is Femoroacetabular Impingement (FAI)?
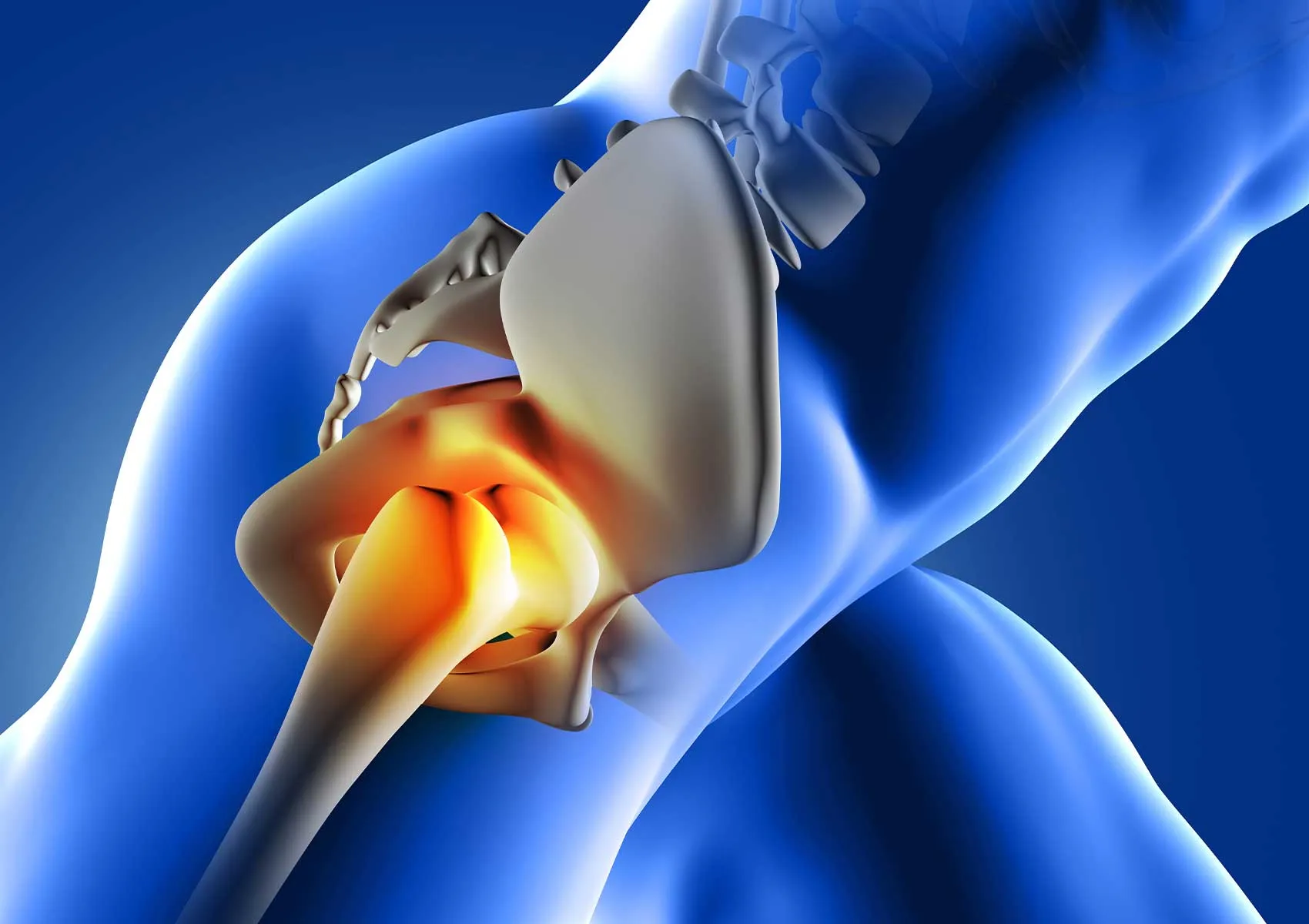
FAI arises from anatomical mismatch between the femoral head (thigh bone) and the acetabulum (pelvic socket). Normally, these structures glide smoothly, but in FAI, bony prominences cause them to collide during movement. This mechanical conflict gradually damages the joint cartilage and the labrum, a cartilage ring that cushions the joint.
Understanding hip anatomy is essential to grasp the condition. Information on labral tears and hip anatomy assists patients in comprehending the disease mechanism. Impingement is often more pronounced during hip flexion and inward rotation movements, with repeated microtraumas deteriorating joint health.
Types of FAI: Cam, Pincer, and Mixed
FAI is classified into three main types, based on the location of the bony deformity, which is important for treatment planning.
1. Cam Type Impingement: Characterized by a bony bump at the femoral head-neck junction. This bump scrapes the cartilage inside the acetabulum during hip movement. It is more common in young men and athletes.
2. Pincer Type Impingement: Occurs when the acetabulum is abnormally deep or retroverted, causing its rim to pinch against the femoral neck and labrum. It tends to be more frequent in middle-aged women.
3. Mixed Type Impingement: A combination of both Cam and Pincer deformities, seen in over 80% of cases.
The structural differences and interaction mechanisms of FAI types are illustrated in the diagram below.
Symptoms of Femoroacetabular Impingement
The hallmark symptom is groin pain, which may radiate to the side of the thigh or rear of the hip. Patients often describe the pain by placing their hand in a "C" shape over the hip (known as the C-sign). Pain typically worsens after prolonged sitting, when getting in and out of a car, or during sports activities.
In addition to pain, restricted hip movement is a significant sign. How hip impingement affects daily life can lower quality of life, making simple tasks like putting on socks or trimming toenails difficult. Some patients may experience snapping sounds or sensations of catching within the joint.
The movement limitations and joint restrictions caused by the condition are visually represented in the illustration below.
Relationship Between FAI and Labral Tears
FAI is a leading cause of labral tears. The labrum is cartilage that stabilizes the hip socket. In FAI, abnormal bone contact continuously compresses and damages the labrum. Chronic trauma may eventually cause the labrum to separate or tear from the bone.
When a labral tear develops, pain becomes sharper and mechanical symptoms such as catching or locking may increase. Labral damage disrupts the joint’s seal and fluid balance, accelerating cartilage deterioration.
The mechanism of labral tear formation due to impingement is explained in the schematic below.
Importance of Early Diagnosis
Early diagnosis in femoroacetabular impingement is vital to preserving the hip joint. Since the condition is progressive, untreated cases may suffer irreversible cartilage damage (osteoarthritis). Detecting the disorder in early stages allows bony corrective procedures that protect the cartilage and enable patients to live pain-free with their own joint long-term.
In advanced cases with widespread cartilage damage, joint-preserving surgeries are less successful and hip replacement may be necessary in later years. Therefore, young, active individuals experiencing groin pain are advised to consult a specialist without delay.
How is FAI Diagnosed?
Diagnosis starts with a detailed patient history and physical examination. The physician performs provocative tests (such as the FADIR test) by positioning the hip in various ways to reproduce impingement symptoms. Pain induced during these tests strengthens suspicion of FAI.
The physical examination maneuvers and test positions used for diagnosis are shown in the image below.
Radiological imaging is used to confirm diagnosis and guide treatment planning:
- X-ray: The first-line imaging to assess bone structures, detect Cam or Pincer deformities, and evaluate joint space.
- MRI (Magnetic Resonance Imaging): The most effective method to visualize labral tears, cartilage damage, and soft tissues in detail. MR arthrography may be performed by injecting contrast into the joint if needed.
- CT Scan (Computed Tomography): Used for 3D evaluation of bone anatomy and surgical planning.
Typical imaging examples of FAI findings are illustrated below.
Treatment Options for FAI: Conservative and Surgical Approaches
Treatment decisions depend on symptom severity, extent of joint damage, and patient expectations.
Conservative Treatment: For patients with mild symptoms or no cartilage damage, non-surgical measures are tried first. These include activity modification (avoiding painful movements), anti-inflammatory medications, and physiotherapy. Detailed information on femoroacetabular impingement can help patients understand their options better.
Surgical Treatment: Surgery is indicated if conservative therapy fails or mechanical symptoms are prominent. Hip arthroscopy is the current gold standard treatment.
- Hip Arthroscopy: A minimally invasive procedure using a camera and small instruments inserted into the joint. Arthroscopic treatment of femoroacetabular impingement involves shaving down bony protrusions (osteoplasty) and repairing torn labrum. This technique offers quicker recovery due to minimal invasiveness. Applications of hip arthroscopy are not limited to impingement but include other intra-articular pathologies.
- Open Surgery / Safe Dislocation: Rarely required for severe deformities.
- Osteotomy: Used to reorient the acetabulum in cases like dysplasia by cutting and repositioning bone. Advanced osteoarthritis may lead to hip replacement surgery. Differences between osteotomy and prosthesis surgery are evaluated based on patient condition.
Treatment pathways are summarized in the flowchart below.
Rehabilitation and Recovery
Postoperative rehabilitation is as critical as the surgery itself for successful outcomes. After arthroscopy, patients typically begin walking with crutches on the same or next day. Initial movement restrictions apply during the first weeks. A personalized physiotherapy program progressively strengthens muscles and improves range of motion. Rehabilitation following femoroacetabular impingement should be tailored and supervised by the physician. Return to sports generally takes 4-6 months, depending on the procedure performed.
This content is intended for informational purposes only and does not substitute professional medical advice, diagnosis, or treatment. Always consult your physician or a qualified healthcare professional regarding any health concerns. The information provided in this article should not be used to create a personal treatment plan. Medical conditions may vary between individuals. Do not delay seeking medical care based on this content.
FAQ
-
What is femoroacetabular impingement (FAI)?
FAI occurs when the bones forming the hip joint (the femoral head and acetabulum) have an abnormal shape, causing them to rub against each other during movement. This can lead to joint damage. It most often affects young, active individuals and may limit the hip's range of motion.
-
What are the main symptoms of FAI?
The primary symptoms include pain in the groin area, restricted hip movement, and increased discomfort after sitting for long periods, driving, or physical activity. Pain may worsen over time, potentially causing difficulty walking and limping.
-
How is femoroacetabular impingement diagnosed?
Diagnosis involves a thorough physical examination by a specialist, evaluation of your symptoms, and imaging tests like X-rays or MRI. Early diagnosis is important to prevent permanent joint damage and labral tears.
-
Can FAI cause a labral tear?
Yes, repeated bone impingement can cause the labrum, the cartilage lining the hip joint, to become compressed and eventually tear. Such tears can increase pain and negatively affect the long-term health of the hip joint.
-
How is femoroacetabular impingement treated?
Treatment depends on the severity of symptoms. Initially, physical therapy and activity modifications may be recommended. In advanced cases or if a labral tear is present, arthroscopic surgery can reshape the bone to relieve impingement. It is essential to consult a specialist for appropriate treatment options.